If you were going to bet on which element of our mountain trek is most likely to keep us off the summit, put your money on altitude sickness. AMS doesn’t care if you’re fit, experienced, or stubborn as a mule. It also isn’t impressed that you just spent a sizeable chunk of your annual income, crossed the wine-dark sea, and changed flights on two continents just to get to the base of the mountain. AMS is utterly indifferent to human ambition. And that makes me nervous.
 Mountaineer's Little Helper.
Mountaineer's Little Helper. Monica and I want better odds. We want an edge. Even if it’s pharmacological.
Enter a drug called Diamox. No, Diamox wasn’t invented for mountaineers. It was concocted to treat glaucoma, a condition in which the pressure inside one’s eyeballs is too high (Marty Feldman Syndrome). It’s also a stimulant, which means that it peps you up. And it’s a mild diuretic, which means that it makes you pee. Despite all that, its main use by far these days is to prevent and treat altitude sickness, even though it says right there on the label that doing so is an unlicensed use of the medicine.
Enter a drug called Diamox. No, Diamox wasn’t invented for mountaineers. It was concocted to treat glaucoma, a condition in which the pressure inside one’s eyeballs is too high (Marty Feldman Syndrome). It’s also a stimulant, which means that it peps you up. And it’s a mild diuretic, which means that it makes you pee. Despite all that, its main use by far these days is to prevent and treat altitude sickness, even though it says right there on the label that doing so is an unlicensed use of the medicine.
The active ingredient in Diamox is acetazolamide, which, as everyone knows, is a carbonic anhydrase inhibitor. (Duh!) As such, it has become the Mountaineer’s Little Helper because it artificially increases heart rate and respiration, which supports what your body does automatically as you drag it to higher elevations. The promise of Diamox is that it can help you adjust more quickly to extreme altitudes and thereby reduce the nasty effects of climbing too high too fast. For that reason, it’s favored by climbers who are in a hurry, and that raises a question for me and Monica: Do we really need it?
Common side effects of Diamox include tingling hands and feet, dizziness, lightheadedness, and, of course, frequent urges to wiz. Less common (but still not uncommon) side effects include blurred vision, nausea, loss of appetite, headache, and fatigue. See the problem? Those are all symptoms of AMS, the very malady Diamox is intended to prevent.
Common side effects of Diamox include tingling hands and feet, dizziness, lightheadedness, and, of course, frequent urges to wiz. Less common (but still not uncommon) side effects include blurred vision, nausea, loss of appetite, headache, and fatigue. See the problem? Those are all symptoms of AMS, the very malady Diamox is intended to prevent.
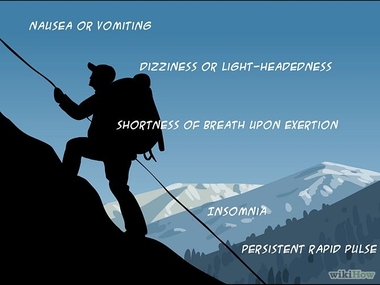 AMS symptoms or Diamox side effects? Answer: Both!
AMS symptoms or Diamox side effects? Answer: Both! And if that doesn’t peg your irony meter, consider this: Diamox also causes photo-toxicity – extreme sensitivity to sunlight. That’s the catchiest of Catch-22s when you recall that we’ll be climbing into the upper troposphere on a mountain situated just 200 miles south of the Equator – up where the sun is so intense that we might as well be hugging a nuclear reactor core.
Ah, but there’s more! Diamox users are urged to contact a doctor if they experience increased body hair (Not making that up!) or an ascension lasting longer than four hours. (Okay, made that one up.)
For these reasons, Mo’ and I are debating whether or not to use the stuff, even though we’ve already purchased it. On the one hand, we shouldn’t need it. The Sierra Club has selected for us the longest route on Kilimanjaro, giving us almost a week to adapt to the altitude. On the other hand, AMS is as fickle as a roulette wheel and is often a trip-ending deal-breaker.
Just in case Deirdre, our trip leader, is listening in on this, let me be precise: Mo’ and I are not deliberating over whether or not to bring Diamox with us; we’re debating whether or not to take the drug prophylactically. Deirdre, whom we are loathe to disappoint, has recommended that we start taking Diamox as soon as we begin trekking. But we are not yet convinced.
Just in case Deirdre, our trip leader, is listening in on this, let me be precise: Mo’ and I are not deliberating over whether or not to bring Diamox with us; we’re debating whether or not to take the drug prophylactically. Deirdre, whom we are loathe to disappoint, has recommended that we start taking Diamox as soon as we begin trekking. But we are not yet convinced.
Not surprisingly, the Internet is no help. Seems like everyone who’s been to Kilimanjaro has a different Diamox story, and stories don’t much impress me. Anecdotal evidence, as they say, is an oxymoron. But there’s also no consensus in the scientific community or even among professional mountaineers about how best to use the drug. In fact, more than a few serious climbers (read purists) even consider Diamox use to be a form of cheating, on a par with hauling oxygen tanks up Everest or doping blood on the Tour de France. But that debate doesn’t concern us. Mo’ and I won’t be stigmatized if an asterisk appears next to our names in the Kilimanjaro record books.*
At this point, we're both still undecided, but Mo' is leaning toward taking Diamox proactively, and I’m leaning toward not taking it unless and until I begin to feel bothersome symptoms of AMS – and by bothersome I mean that they start rivaling the anticipated side effects of the drug itself. I guess that makes me the kind of guy who would wait the full four hours before calling his doctor.
At this point, we're both still undecided, but Mo' is leaning toward taking Diamox proactively, and I’m leaning toward not taking it unless and until I begin to feel bothersome symptoms of AMS – and by bothersome I mean that they start rivaling the anticipated side effects of the drug itself. I guess that makes me the kind of guy who would wait the full four hours before calling his doctor.
* You know, like BARRY B*NDS.








 RSS Feed
RSS Feed

